







Photo: San Ramon Regional Medical Center
Part of statewide protest calling for additional support in the workplace
By Maria Leal, SEIU-United Healthcare Workers West
![]() Healthcare workers across California will picket at 12 Tenet Healthcare facilities to call for additional support in the workplace starting July 11. The pickets will take place at facilities owned by Tenet Healthcare. These workers are part of what is expected to be tens of thousands of healthcare workers picketing this summer. Workers from four Prime Healthcare facilities in Southern California also start their pickets the same day.
Healthcare workers across California will picket at 12 Tenet Healthcare facilities to call for additional support in the workplace starting July 11. The pickets will take place at facilities owned by Tenet Healthcare. These workers are part of what is expected to be tens of thousands of healthcare workers picketing this summer. Workers from four Prime Healthcare facilities in Southern California also start their pickets the same day.
The protest at Tenet San Ramon Regional Medical Center located at 6001 Norris Canyon Road will take place Friday, July 21 from 11:30 am – 1:30 pm.
After years of battling the COVID pandemic, healthcare workers are calling on management to provide additional support to retain and attract more caregivers to the industry.
“We are simply asking for additional support to improve working conditions. We put our lives at risk during the pandemic and were called ‘heroes,” said Bridgette Lamere, Respiratory Therapist, Tenet Emmanuel Medical Center in Turlock. “We are calling on our employers to increase their investments in workers to ensure the additional support of healthcare workers, our patients, and our entire communities.”
SEIU-United Healthcare Workers West (SEIU-UHW) is a healthcare justice union of more than 100,000 healthcare workers, patients, and healthcare activists united to ensure affordable, accessible, high-quality care for all Californians, provided by valued and respected healthcare workers. Learn more at www.seiu-uhw.org.
Efforts to reach the media relationships staff for the San Ramon Regional Medical Center were unsuccessful prior to publication time. Please check back for any updates.
Allen D. Payton contributed to this report.
Read More
By Lt. Holley Connors, Walnut Creek Police Department
On July 3rd, at 1:21 p.m., a 911 caller reported a vehicle collided with a pedestrian on Ygnacio Valley Road, east of the intersection at Lennon Lane. Officers arrived and found a male pedestrian conscious, but with significant injuries. Preliminary details indicated the driver’s vehicle drifted to the right, hopped the curb, and struck the pedestrian who was doing maintenance work at that location. The driver of the vehicle was uninjured.
Officers and AMR personnel provided medical aid to the pedestrian before he was transported to the hospital. Unfortunately, the pedestrian later succumbed to his injuries. The driver remained on scene and cooperated with responding officers.
According to Bay City News, the victim was identified by the Contra Costa County Coroner’s Office as Cornelio Tovar Sanchez, age 54 of Antioch.
The cause of this accident is under investigation. If you have any information about this case, please contact Walnut Creek PD Dispatch at 925-935-6400.
Allen D. Payton contributed to this report.
Read More

Nighttime construction on the Mokelumne Trail Overcrossing will occur this weekend. Photo: CCTA
Between Lone Tree Way and Sand Creek Road Saturday, July 8 through Sunday, July 9, 2023
For Mokelumne Trail Overcrossing construction
By Ivan Ramirez, Contra Costa Transportation Authority
BRENTWOOD, CA – In partnership with the City of Brentwood, the Contra Costa Transportation Authority (CCTA) is constructing the Mokelumne Trail Bicycle and Pedestrian Overcrossing to provide safe access to cyclists and pedestrians for commuting and recreational travel, reconnecting two sides of the trail that were separated by the expansion of State Route 4.
This overnight closure will facilitate the removing of the temporary structure that was used to support the bridge and will impact State Route 4 in the eastbound direction. CCTA and the California Department of Transportation (Caltrans) have scheduled the closure during the early morning hours in order to minimize impacts to the motoring public.
In order to ensure crew and public safety during the planned construction work, a temporary nighttime freeway closure in the eastbound direction of State Route 4 will occur between Saturday, July 8 and Sunday, July 9, 2023 on the following schedule (weather permitting):
Eastbound Highway 4 will be closed between Lone Tree Way and Sand Creek Road from 9:00 p.m. on Saturday, July 8 until 7:00 a.m. on Sunday, July 9, 2023.
DetoursDetours will be in place to reroute drivers around the closure and are planned as follows:
Eastbound traffic will be directed to exit at Lone Tree Way, go eastbound to Shady Willow Lane, then southbound on Shady Willow Lane to Sand Creek Road, before proceeding westbound on Sand Creek Road to the eastbound State Route 4 on-ramp.
Future Freeway Closures
Additional overnight closures will be needed over the course of the next several weeks (weather dependent) to facilitate construction work of the future Mokelumne Trail Bicycle and Pedestrian Overcrossing. Additional information regarding dates and detours will be provided once the schedule is confirmed. This project is anticipated to be complete in late summer or early fall of 2023.About the Contra Costa Transportation Authority
The Contra Costa Transportation Authority (CCTA) is a public agency formed by Contra Costa voters in 1988 to manage the county’s transportation sales tax program and oversee countywide transportation planning efforts. With a staff of twenty people managing a multi-billion-dollar suite of projects and programs, CCTA is responsible for planning, funding and delivering critical transportation infrastructure projects and programs that connect our communities, foster a strong economy, increase sustainability, and safely and efficiently get people where they need to go. CCTA also serves as the county’s designated Congestion Management Agency, responsible for putting programs in place to keep traffic levels manageable. More information about CCTA is available at ccta.net.
Read More
More than 11 million arrest and conviction records automatically cleared including old arrests that never turned into charges and provides relief to people who completed all conditions of their sentence
Due to legislation pioneered by Los Angeles DA George Gascón
By Max Szabo, Prosecutors Alliance of California
![]() SACRAMENTO–New data from the California Department of Justice (CAL DOJ) indicates that 11,164,458 records of arrest and conviction were automatically cleared between July 1, 2022 and December 31, 2022 pursuant to Assembly Bill 1076. The historic reform automated a process that individuals were already entitled to but had to seek out through an arduous process. AB 1076 requires CAL DOJ to automatically clear old arrests that never turned into charges and provides relief to people who completed all the conditions of their sentence, thereby expanding education, employment and housing opportunities for countless Californians.
SACRAMENTO–New data from the California Department of Justice (CAL DOJ) indicates that 11,164,458 records of arrest and conviction were automatically cleared between July 1, 2022 and December 31, 2022 pursuant to Assembly Bill 1076. The historic reform automated a process that individuals were already entitled to but had to seek out through an arduous process. AB 1076 requires CAL DOJ to automatically clear old arrests that never turned into charges and provides relief to people who completed all the conditions of their sentence, thereby expanding education, employment and housing opportunities for countless Californians.
“People who were arrested or convicted of low-level crimes and did what was asked of them are entitled to a second chance under the law, but bureaucratic barriers kept them in a paper prison,” said Cristine DeBerry, Founder and Executive Director of the Prosecutors Alliance of California. “That wasn’t just unfair, it was unsafe, as a criminal record hangs over people, hampering their access to employment and housing opportunities, primary factors that drive recidivism. The system had taken away hope and opportunity, but commonsense and technology enabled one of the most important reforms in years.”
The automated record clearance is due to a 2019 law, Assembly Bill 1076, which was authored by Phil Ting (D-San Francisco) and sponsored by then-San Francisco District Attorney George Gascón. The legislation mandated that the state Department of Justice automatically clear records of arrests that did not result in a conviction after the statute of limitations had passed as well as convictions involving probation and jail once an offender’s sentence was completed. Individuals sentenced to prison and anyone who had to register as a sex offender or who violated their probation is not eligible. The record clearance largely benefits individuals who had committed drugs or property crimes.
“It’s a vicious cycle, as communities of color are more likely to be arrested, they are therefore more likely to have a record that includes an arrest or conviction, and yet they were less likely to be aware that they were entitled to relief,” said LA County District Attorney George Gascón. “These were unnecessary barriers that make it more difficult to successfully reenter and break the cycle by limiting access to jobs, education and housing. Breaking down these barriers makes our system more just and our communities more safe.”
During the appropriations process that bill was limited to prospective arrests and convictions. However, a subsequent effort in 2021, AB 1038, authored again by Assemblymember Ting, and sponsored by the Prosecutors Alliance of California, made the record clearance provided under AB 1076 retroactive. That bill took effect July 1, 2023. The newly released DOJ data indicates that the relief granted thus far was pursuant to AB 1076, the initial authorizing legislation only, suggesting that the expanded eligibility profile now in effect under AB 1038 will result in the clearance of millions of additional records.
Prior to the automated record clearance, 8 million California residents had criminal convictions on their records that hampered their ability to find work and housing, secure public benefits, or even get admitted to college. Studies indicate approximately two million of them were eligible for record clearance. Millions more have old arrests on their record that never resulted in a conviction but, remain as obstacles to employment.
Under the law arrests that didn’t result in a conviction may be cleared. Convictions that carry probation or jail time are also eligible for record clearance after the individual completes all the terms and conditions of their sentence. Prior to AB 1076, however, this required individuals to be aware of their eligibility and to retain an attorney to proactively file the necessary petition. As a result, millions of Californians have been entitled to relief for years that they never realized because they had to jump through hoops to get it. In fact, nationally, only 6.5% of eligible people have been estimated to obtain record clearance within five years of eligibility. With more affluent communities more able to afford a private attorney, this bureaucracy disproportionately impacted socioeconomically disadvantaged communities and communities of color in particular.
Nearly 90% of employers, 80% of landlords, and 60% of colleges screen applicants’ criminal records. According to a 2012 study conducted by the Society for Human Resource Management, many prospective employees and housing applicants are rejected solely based on having an arrest record on file. Studies also show people with unsealed arrest records have a substantially increased chance of living in poverty, earning lower wages, with fewer educational opportunities.
The concept for the legislation grew out of DA Gascón’s effort to clear old cannabis convictions that were eligible for clearance pursuant to Proposition 64. That effort has now been adopted by prosecutors’ offices across the nation. Notably, the algorithm that enabled automated record clearance pursuant to AB 1076–much like the cannabis clearance effort–would not be possible without the help and support of Code For America. Research by the California Policy Lab of the University of California provided supporting evidence regarding the feasibility of large-scale record clearance automation, as well as its enormous potential impact on the lives of Californians. Assemblymember Phil Ting has the sincere gratitude of the Prosecutors Alliance for leading the historic initiative and seeing that all eligible and impacted Californians would obtain the relief to which they are entitled.
The Prosecutors Alliance of California is fiscally sponsored by Tides Advocacy, a social welfare organization. Contra Costa District Attorney Diana Becton is a founding member. For more information about the Prosecutors Alliance go to www.ProsecutorsAlliance.org and keep up with our work on Twitter, Instagram and Facebook.
Read More
Source: Con Fire
Limited response plan implementation ensures responses to exceptionally high volume of fireworks-caused fires
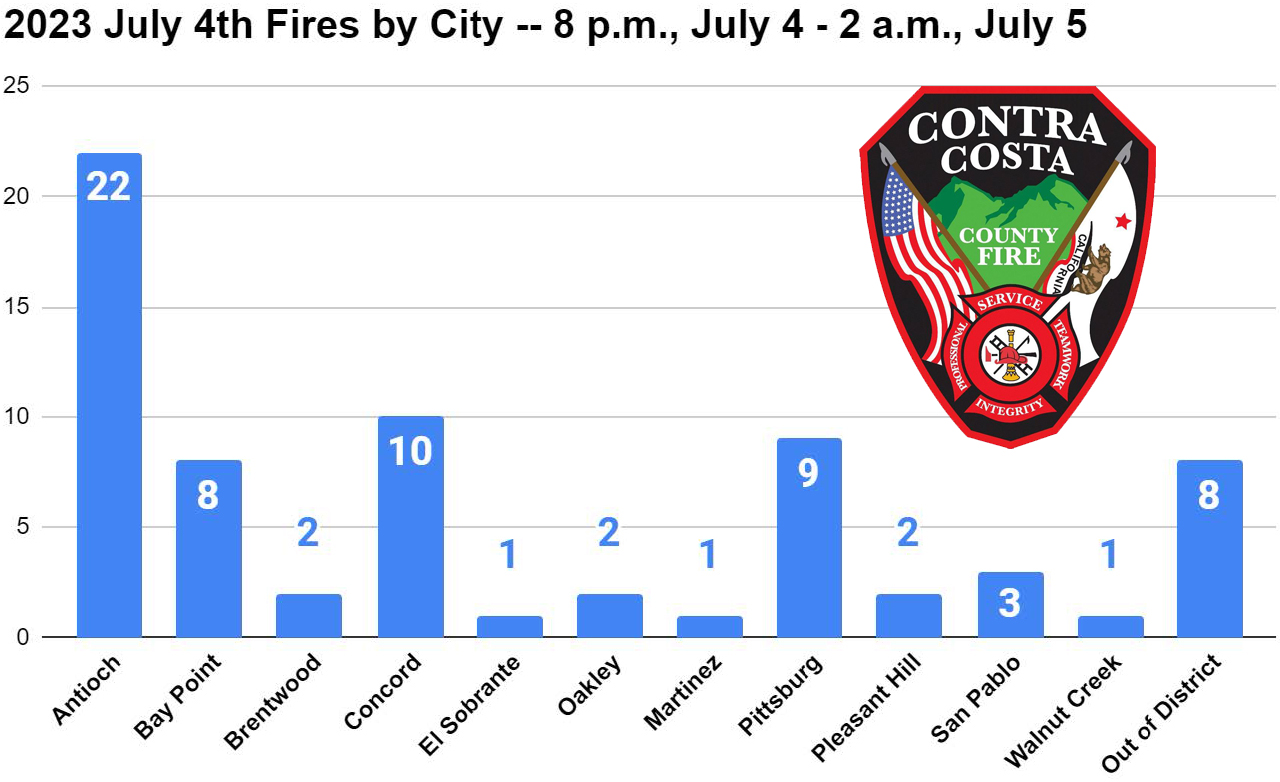
Antioch had most with 22 & worst structure fire destroying garage, damaging two homes in which four residents displaced, dog died
Martinez man loses part of hand holding an exploding firework
By Steve Hill, PIO, Contra Costa County Fire Protection District
July 6, 2023 – Contra Costa County Fire Protection District today made available details of the fire and EMS activity, much of it fireworks related, occurring across the district on the Independence Day holiday evening.
For the six-hour period from 8 p.m., July 4, to 2 a.m., July 5, the district dispatched crews to 69 fire incidents. This represents a more than 400 percent increase over other recent Tuesdays, which in June, averaged 20 fire dispatches for the entire day. Year-over-year, fire incidents were up nearly 60 percent.
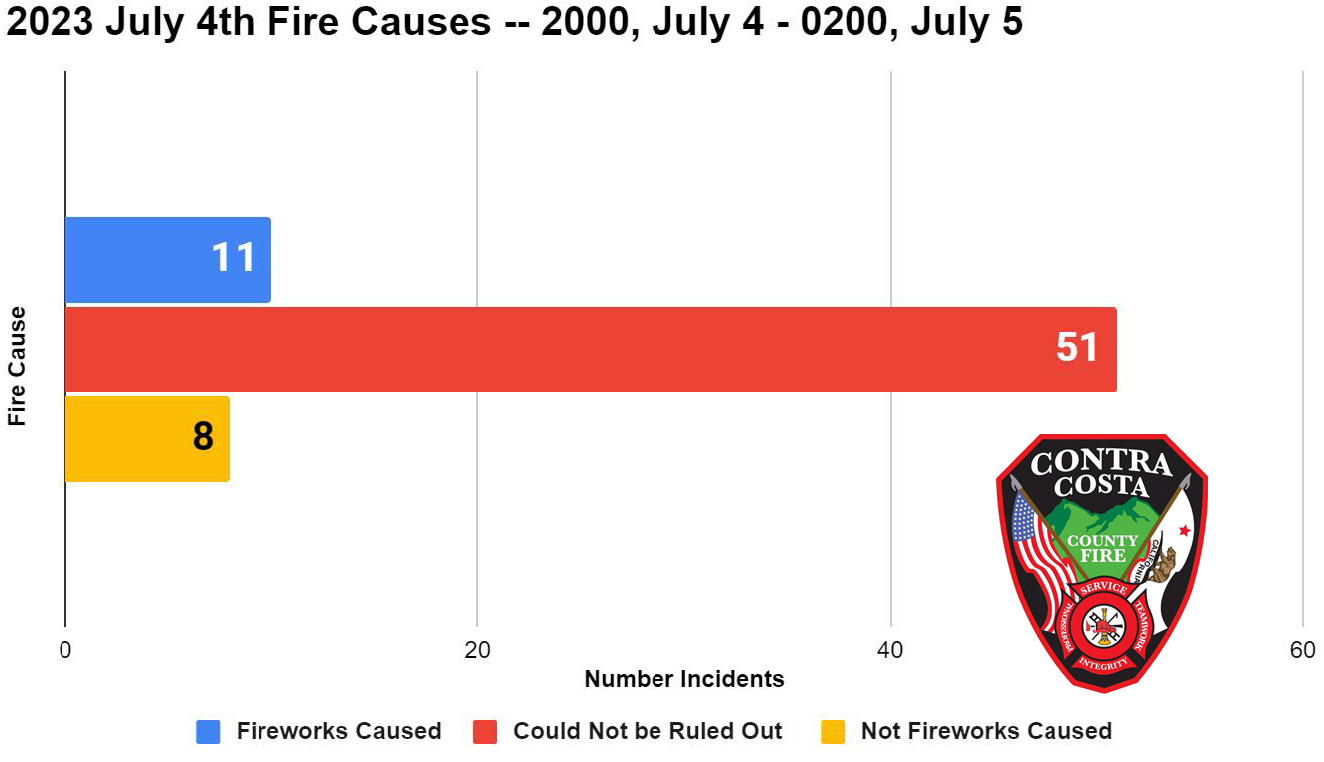
The holiday evening’s 69 fire incidents point to the dangers of fireworks use in current heightened fire danger conditions. Eleven of these fires are known to have been caused, and another 51 suspected of having been caused by fireworks.
Source: Con Fire
While the cool weather was favorable and the midweek timing had the holiday falling on a work night, fires numbered some 60 percent more than 4th of July 2023’s 44 fire incidents for the same evening period.
Four Residents Displaced, Dog Dies in Antioch Fire
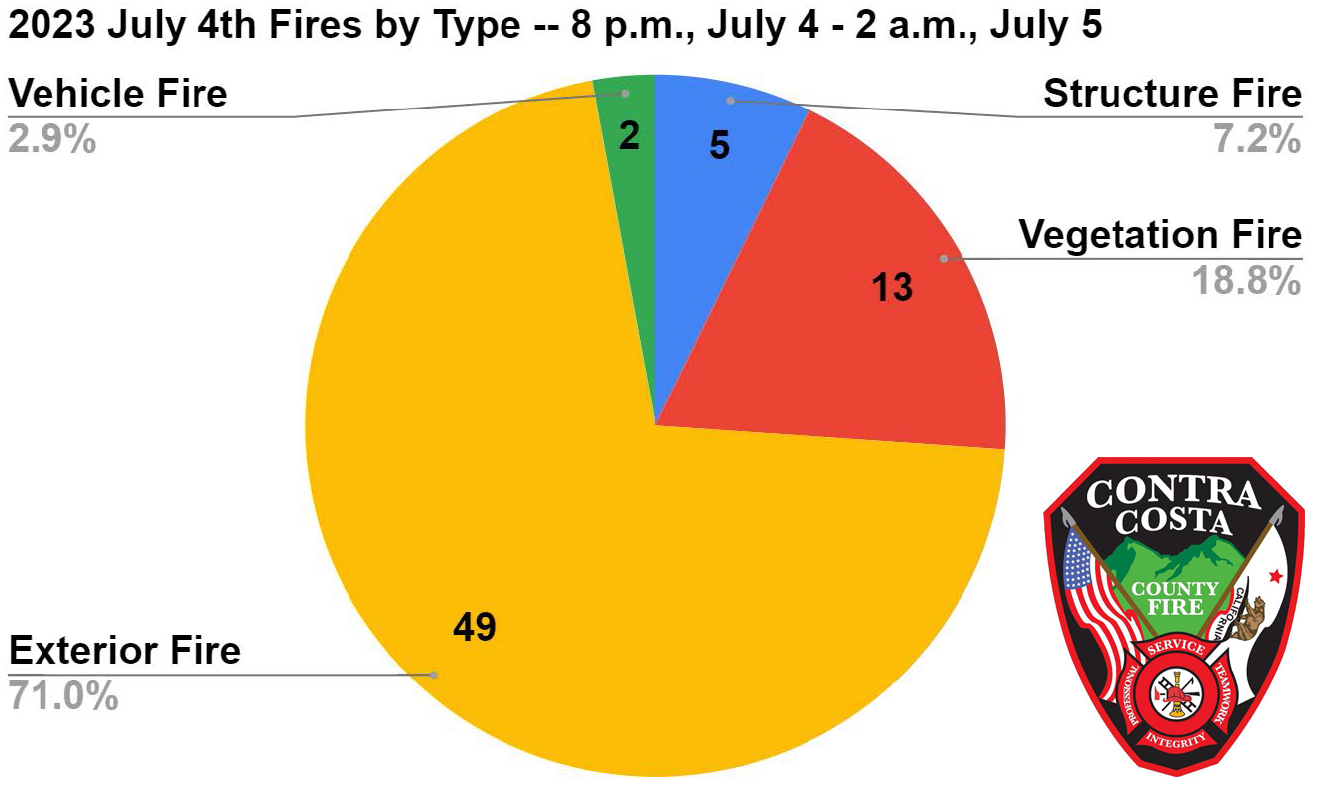
In spite of more than 60 grass, vegetation and other exterior fires burning across the district on theevening of the Fourth, only four structure fires ensued. Of these, in three cases, fireworks could not be ruled out as the cause. In the worst structure fire of the evening, in the 2 a.m. hour in Antioch, a garage was destroyed, and two adjacent homes substantially damaged as a result of fireworks. In all, four residents were displaced, and a dog died, as a result of this unnecessary fire.
20% Increase in Emergency Medical Service Incidents
Calls for emergency medical services were also up over normal, non-holiday periods with some of this increase likely attributable to fireworks activity. On the Fourth, 240 EMS incidents were dispatched with 64 of these occurring between 8 p.m. and 2 a.m. the next day. Total EMS responses represent about a 20% increase over more typical weekdays. On average, Con Fire responds to just over 200 EMS incidents daily.
In one particularly egregious case, a 66-year-old male in Martinez was gravely injured in the 10 p.m. hour when he lost part of a hand while holding an exploding firework.
Source: Con Fire
Considerable preparation across the district, including upstaffing of additional dispatchers; two hand crews and equipment; two fire dozers; and the district operations center, staffed by multiple chief officers; resulted in rapid and overwhelming responses, which served to limit fire spread, and resultant damage when fires did occur.
All 60-plus grass and exterior fires were kept small, limiting potential for structure damage as a result of rapid and overwhelming responses as well as early notifications to 911 by residents.
Read More

The Jazz, Blues, and Funk Festival is BACK!
Join us at the Pittsburg Civic Center for the Jazz, Blues, Funk Festival the weekend of August 19-20. The Festival is a two-day event that will feature a variety of artists, food, beer, and wine.
Tickets are on sale now with the option for VIP, General admission, and Two-day Passes.
Buy your tickets now: www.pittsburgtickets.com
Read More
By Mashie Goldshmid, Program Director, Chabad of the Delta
With gratitude to G-d, we are excited to share that Chabad has just leased a new space to serve as the Jewish Center of East Contra Costa. The grand opening celebration will take place on Sunday, July 16 at 9:30am, inviting families and friends to join in the festivities.
The grand opening event promises an exciting lineup of activities for attendees of all ages. Live music performances, engaging kids’ entertainment, and a delectable dairy buffet are among the highlights that will contribute to the festive atmosphere. The celebration embodies the spirit of growth and community, inviting everyone to participate and rejoice together.
The new Chabad Jewish Center symbolizes a space where the East Contra Costa Jewish community can thrive collectively, creating an environment that encourages unity and embraces Jewish traditions. To RSVP visit JewishDelta.com/GrandOpening
Read More
Poor choices behind the wheel result in tragedy on California’s roadways
By Jaime Coffee, CHP Media Relations
SACRAMENTO, Calif. – The results of the California Highway Patrol’s (CHP) recent Independence Day Maximum Enforcement Period (MEP) are a sobering reminder of the consequences resulting from unsafe driving behaviors.
Sixty-eight people were killed in crashes throughout the state during the Independence Day MEP, which began at 6:01 p.m. on Friday, June 30, and concluded at 11:59 p.m. on Tuesday, July 4. Tragically, nearly half of the total number of vehicle occupants who died within CHP jurisdiction were not wearing a seat belt.
With unsafe speed being the number one contributor to crashes in California, the CHP placed a special emphasis on its enforcement during the recent MEP. CHP officers issued more than 9,700 speed citations throughout the long Independence Day weekend.
Additionally, impaired drivers were removed from California’s roadways at an alarming rate during the holiday enforcement effort. CHP officers made 1,224 arrests for driving under the influence, which is an average of one DUI arrest every five minutes.
“The results of this MEP are concerning and reinforce the need for responsible behavior behind the wheel,” said CHP Commissioner Sean Duryee. “All of these deaths were preventable, and the loved ones they leave behind will be forever impacted. Traffic safety is everyone’s responsibility, and these statistics show us how much work there is still to be done. The CHP is committed to making California’s roadways safer for all who use them.”
To help protect those who are traveling on California’s roadways during the holidays, the CHP implements six MEPs per year. The next MEP is scheduled for Labor Day weekend. Throughout the holiday weekend, all available uniformed members of the Department will be on patrol to enhance public safety, deter unsafe driving behavior, and, when necessary, take appropriate enforcement action.
Keep yourself and others who are on the road safe by buckling up, driving at a speed safe for conditions, avoid distractions behind the wheel, and always designating a sober driver.
The mission of the CHP is to provide the highest level of Safety, Service, and Security.
Read More
Enjoy parks safely and responsibly; no fireworks allowed in Regional Parks
The East Bay Regional Park District is urging Fourth of July visitors to enjoy parks safely and responsibly.
The Fourth of July holiday is typically one of the busiest days of the year for Regional Parks. Some of our more popular parks and swim areas are expected to reach capacity early in the day. Visitors are encouraged to carpool and arrive early. Parking lots may become full, though there are many Regional Park options to consider.
When visiting a Regional Park on the Fourth of July, visitors should know and follow these important tips and rules.
- NO Fireworks – Fireworks are not allowed in Regional Parks.
- Stay Cool and Hydrated – Plan ahead and bring plenty of water.
- Beat the Heat – With hot weather, visit in the morning and early evening when it is cooler. If you do venture out, wear a hat and loose, lightweight, and light-colored clothing.
- Drink Responsibly – Drinking alcohol is only allowed at certain Regional Parks. Check www.ebparks.org/parks before you go.
- Follow Water Safety Rules if Swimming – Free loaner life jackets are available at all East Bay Regional Park District swim facilities as an extra safeguard for anyone concerned about their swimming abilities or their children.
- Be Fire Smart – Be aware of Red Flag warnings, fire danger levels, and fire safety rules. www.ebparks.org/public-safety/fire/fire-danger-levels-restrictions.
The East Bay Regional Park District is the largest regional park system in the nation, comprising 73 parks, 55 miles of shoreline, and over 1,300 miles of trails for hiking, biking, horseback riding, and environmental education. The Park District receives more than 25 million visits annually throughout Alameda and Contra Costa counties in the San Francisco Bay Area.
Read More
By City of Pinole
The City of Pinole will not be hosting fireworks this year.
We encourage residents to enjoy a safe and fun Fourth of July, celebrating the birth of our exceptional nation. Families and friends often gather to recognize this special day together.
For a number of years, until 2010, the City hosted a fireworks display at Bayfront Park on Fourth of July. The City had been hoping to again host fireworks on Fourth of July in 2023. After collaborating with partner agencies to assess Bayfront Park and other sites, it was determined that there is no safe and accessible site in Pinole from which to launch fireworks. Since Pinole last held fireworks, fireworks safety standards and practices have evolved and concern about wildfires has increased substantially.
For those who would like to see fireworks, below is a list of events in Pinole’s neighboring cities.
3rd of July Fireworks
Richmond: Richmond Marina Bay Park, fireworks begin at 9:15 p.m.
Fourth of July Fireworks
Antioch: Fireworks in downtown Antioch over the San Joaquin River, start at after dusk
Concord: Mt. Diablo High School, at around 9 p.m.
Hercules: Bayfront Blvd, the show will start once it’s dark
Pleasant Hill: College Park High School fields, fireworks around 8:45 p.m.
Read More








Photo: San Ramon Regional Medical Center
Part of statewide protest calling for additional support in the workplace
By Maria Leal, SEIU-United Healthcare Workers West
![]() Healthcare workers across California will picket at 12 Tenet Healthcare facilities to call for additional support in the workplace starting July 11. The pickets will take place at facilities owned by Tenet Healthcare. These workers are part of what is expected to be tens of thousands of healthcare workers picketing this summer. Workers from four Prime Healthcare facilities in Southern California also start their pickets the same day.
Healthcare workers across California will picket at 12 Tenet Healthcare facilities to call for additional support in the workplace starting July 11. The pickets will take place at facilities owned by Tenet Healthcare. These workers are part of what is expected to be tens of thousands of healthcare workers picketing this summer. Workers from four Prime Healthcare facilities in Southern California also start their pickets the same day.
The protest at Tenet San Ramon Regional Medical Center located at 6001 Norris Canyon Road will take place Friday, July 21 from 11:30 am – 1:30 pm.
After years of battling the COVID pandemic, healthcare workers are calling on management to provide additional support to retain and attract more caregivers to the industry.
“We are simply asking for additional support to improve working conditions. We put our lives at risk during the pandemic and were called ‘heroes,” said Bridgette Lamere, Respiratory Therapist, Tenet Emmanuel Medical Center in Turlock. “We are calling on our employers to increase their investments in workers to ensure the additional support of healthcare workers, our patients, and our entire communities.”
SEIU-United Healthcare Workers West (SEIU-UHW) is a healthcare justice union of more than 100,000 healthcare workers, patients, and healthcare activists united to ensure affordable, accessible, high-quality care for all Californians, provided by valued and respected healthcare workers. Learn more at www.seiu-uhw.org.
Efforts to reach the media relationships staff for the San Ramon Regional Medical Center were unsuccessful prior to publication time. Please check back for any updates.
Allen D. Payton contributed to this report.
Read More
By Lt. Holley Connors, Walnut Creek Police Department
On July 3rd, at 1:21 p.m., a 911 caller reported a vehicle collided with a pedestrian on Ygnacio Valley Road, east of the intersection at Lennon Lane. Officers arrived and found a male pedestrian conscious, but with significant injuries. Preliminary details indicated the driver’s vehicle drifted to the right, hopped the curb, and struck the pedestrian who was doing maintenance work at that location. The driver of the vehicle was uninjured.
Officers and AMR personnel provided medical aid to the pedestrian before he was transported to the hospital. Unfortunately, the pedestrian later succumbed to his injuries. The driver remained on scene and cooperated with responding officers.
According to Bay City News, the victim was identified by the Contra Costa County Coroner’s Office as Cornelio Tovar Sanchez, age 54 of Antioch.
The cause of this accident is under investigation. If you have any information about this case, please contact Walnut Creek PD Dispatch at 925-935-6400.
Allen D. Payton contributed to this report.
Read More
Nighttime construction on the Mokelumne Trail Overcrossing will occur this weekend. Photo: CCTA
Between Lone Tree Way and Sand Creek Road Saturday, July 8 through Sunday, July 9, 2023
For Mokelumne Trail Overcrossing construction
By Ivan Ramirez, Contra Costa Transportation Authority
BRENTWOOD, CA – In partnership with the City of Brentwood, the Contra Costa Transportation Authority (CCTA) is constructing the Mokelumne Trail Bicycle and Pedestrian Overcrossing to provide safe access to cyclists and pedestrians for commuting and recreational travel, reconnecting two sides of the trail that were separated by the expansion of State Route 4.
This overnight closure will facilitate the removing of the temporary structure that was used to support the bridge and will impact State Route 4 in the eastbound direction. CCTA and the California Department of Transportation (Caltrans) have scheduled the closure during the early morning hours in order to minimize impacts to the motoring public.
In order to ensure crew and public safety during the planned construction work, a temporary nighttime freeway closure in the eastbound direction of State Route 4 will occur between Saturday, July 8 and Sunday, July 9, 2023 on the following schedule (weather permitting):
Eastbound Highway 4 will be closed between Lone Tree Way and Sand Creek Road from 9:00 p.m. on Saturday, July 8 until 7:00 a.m. on Sunday, July 9, 2023.
DetoursDetours will be in place to reroute drivers around the closure and are planned as follows:
Eastbound traffic will be directed to exit at Lone Tree Way, go eastbound to Shady Willow Lane, then southbound on Shady Willow Lane to Sand Creek Road, before proceeding westbound on Sand Creek Road to the eastbound State Route 4 on-ramp.
Future Freeway Closures
Additional overnight closures will be needed over the course of the next several weeks (weather dependent) to facilitate construction work of the future Mokelumne Trail Bicycle and Pedestrian Overcrossing. Additional information regarding dates and detours will be provided once the schedule is confirmed. This project is anticipated to be complete in late summer or early fall of 2023.About the Contra Costa Transportation Authority
The Contra Costa Transportation Authority (CCTA) is a public agency formed by Contra Costa voters in 1988 to manage the county’s transportation sales tax program and oversee countywide transportation planning efforts. With a staff of twenty people managing a multi-billion-dollar suite of projects and programs, CCTA is responsible for planning, funding and delivering critical transportation infrastructure projects and programs that connect our communities, foster a strong economy, increase sustainability, and safely and efficiently get people where they need to go. CCTA also serves as the county’s designated Congestion Management Agency, responsible for putting programs in place to keep traffic levels manageable. More information about CCTA is available at ccta.net.
Read More
More than 11 million arrest and conviction records automatically cleared including old arrests that never turned into charges and provides relief to people who completed all conditions of their sentence
Due to legislation pioneered by Los Angeles DA George Gascón
By Max Szabo, Prosecutors Alliance of California
![]() SACRAMENTO–New data from the California Department of Justice (CAL DOJ) indicates that 11,164,458 records of arrest and conviction were automatically cleared between July 1, 2022 and December 31, 2022 pursuant to Assembly Bill 1076. The historic reform automated a process that individuals were already entitled to but had to seek out through an arduous process. AB 1076 requires CAL DOJ to automatically clear old arrests that never turned into charges and provides relief to people who completed all the conditions of their sentence, thereby expanding education, employment and housing opportunities for countless Californians.
SACRAMENTO–New data from the California Department of Justice (CAL DOJ) indicates that 11,164,458 records of arrest and conviction were automatically cleared between July 1, 2022 and December 31, 2022 pursuant to Assembly Bill 1076. The historic reform automated a process that individuals were already entitled to but had to seek out through an arduous process. AB 1076 requires CAL DOJ to automatically clear old arrests that never turned into charges and provides relief to people who completed all the conditions of their sentence, thereby expanding education, employment and housing opportunities for countless Californians.
“People who were arrested or convicted of low-level crimes and did what was asked of them are entitled to a second chance under the law, but bureaucratic barriers kept them in a paper prison,” said Cristine DeBerry, Founder and Executive Director of the Prosecutors Alliance of California. “That wasn’t just unfair, it was unsafe, as a criminal record hangs over people, hampering their access to employment and housing opportunities, primary factors that drive recidivism. The system had taken away hope and opportunity, but commonsense and technology enabled one of the most important reforms in years.”
The automated record clearance is due to a 2019 law, Assembly Bill 1076, which was authored by Phil Ting (D-San Francisco) and sponsored by then-San Francisco District Attorney George Gascón. The legislation mandated that the state Department of Justice automatically clear records of arrests that did not result in a conviction after the statute of limitations had passed as well as convictions involving probation and jail once an offender’s sentence was completed. Individuals sentenced to prison and anyone who had to register as a sex offender or who violated their probation is not eligible. The record clearance largely benefits individuals who had committed drugs or property crimes.
“It’s a vicious cycle, as communities of color are more likely to be arrested, they are therefore more likely to have a record that includes an arrest or conviction, and yet they were less likely to be aware that they were entitled to relief,” said LA County District Attorney George Gascón. “These were unnecessary barriers that make it more difficult to successfully reenter and break the cycle by limiting access to jobs, education and housing. Breaking down these barriers makes our system more just and our communities more safe.”
During the appropriations process that bill was limited to prospective arrests and convictions. However, a subsequent effort in 2021, AB 1038, authored again by Assemblymember Ting, and sponsored by the Prosecutors Alliance of California, made the record clearance provided under AB 1076 retroactive. That bill took effect July 1, 2023. The newly released DOJ data indicates that the relief granted thus far was pursuant to AB 1076, the initial authorizing legislation only, suggesting that the expanded eligibility profile now in effect under AB 1038 will result in the clearance of millions of additional records.
Prior to the automated record clearance, 8 million California residents had criminal convictions on their records that hampered their ability to find work and housing, secure public benefits, or even get admitted to college. Studies indicate approximately two million of them were eligible for record clearance. Millions more have old arrests on their record that never resulted in a conviction but, remain as obstacles to employment.
Under the law arrests that didn’t result in a conviction may be cleared. Convictions that carry probation or jail time are also eligible for record clearance after the individual completes all the terms and conditions of their sentence. Prior to AB 1076, however, this required individuals to be aware of their eligibility and to retain an attorney to proactively file the necessary petition. As a result, millions of Californians have been entitled to relief for years that they never realized because they had to jump through hoops to get it. In fact, nationally, only 6.5% of eligible people have been estimated to obtain record clearance within five years of eligibility. With more affluent communities more able to afford a private attorney, this bureaucracy disproportionately impacted socioeconomically disadvantaged communities and communities of color in particular.
Nearly 90% of employers, 80% of landlords, and 60% of colleges screen applicants’ criminal records. According to a 2012 study conducted by the Society for Human Resource Management, many prospective employees and housing applicants are rejected solely based on having an arrest record on file. Studies also show people with unsealed arrest records have a substantially increased chance of living in poverty, earning lower wages, with fewer educational opportunities.
The concept for the legislation grew out of DA Gascón’s effort to clear old cannabis convictions that were eligible for clearance pursuant to Proposition 64. That effort has now been adopted by prosecutors’ offices across the nation. Notably, the algorithm that enabled automated record clearance pursuant to AB 1076–much like the cannabis clearance effort–would not be possible without the help and support of Code For America. Research by the California Policy Lab of the University of California provided supporting evidence regarding the feasibility of large-scale record clearance automation, as well as its enormous potential impact on the lives of Californians. Assemblymember Phil Ting has the sincere gratitude of the Prosecutors Alliance for leading the historic initiative and seeing that all eligible and impacted Californians would obtain the relief to which they are entitled.
The Prosecutors Alliance of California is fiscally sponsored by Tides Advocacy, a social welfare organization. Contra Costa District Attorney Diana Becton is a founding member. For more information about the Prosecutors Alliance go to www.ProsecutorsAlliance.org and keep up with our work on Twitter, Instagram and Facebook.
Read More
Source: Con Fire
Limited response plan implementation ensures responses to exceptionally high volume of fireworks-caused fires
Antioch had most with 22 & worst structure fire destroying garage, damaging two homes in which four residents displaced, dog died
Martinez man loses part of hand holding an exploding firework
By Steve Hill, PIO, Contra Costa County Fire Protection District
July 6, 2023 – Contra Costa County Fire Protection District today made available details of the fire and EMS activity, much of it fireworks related, occurring across the district on the Independence Day holiday evening.
For the six-hour period from 8 p.m., July 4, to 2 a.m., July 5, the district dispatched crews to 69 fire incidents. This represents a more than 400 percent increase over other recent Tuesdays, which in June, averaged 20 fire dispatches for the entire day. Year-over-year, fire incidents were up nearly 60 percent.
The holiday evening’s 69 fire incidents point to the dangers of fireworks use in current heightened fire danger conditions. Eleven of these fires are known to have been caused, and another 51 suspected of having been caused by fireworks.
Source: Con Fire
While the cool weather was favorable and the midweek timing had the holiday falling on a work night, fires numbered some 60 percent more than 4th of July 2023’s 44 fire incidents for the same evening period.
Four Residents Displaced, Dog Dies in Antioch Fire
In spite of more than 60 grass, vegetation and other exterior fires burning across the district on theevening of the Fourth, only four structure fires ensued. Of these, in three cases, fireworks could not be ruled out as the cause. In the worst structure fire of the evening, in the 2 a.m. hour in Antioch, a garage was destroyed, and two adjacent homes substantially damaged as a result of fireworks. In all, four residents were displaced, and a dog died, as a result of this unnecessary fire.
20% Increase in Emergency Medical Service Incidents
Calls for emergency medical services were also up over normal, non-holiday periods with some of this increase likely attributable to fireworks activity. On the Fourth, 240 EMS incidents were dispatched with 64 of these occurring between 8 p.m. and 2 a.m. the next day. Total EMS responses represent about a 20% increase over more typical weekdays. On average, Con Fire responds to just over 200 EMS incidents daily.
In one particularly egregious case, a 66-year-old male in Martinez was gravely injured in the 10 p.m. hour when he lost part of a hand while holding an exploding firework.
Source: Con Fire
Considerable preparation across the district, including upstaffing of additional dispatchers; two hand crews and equipment; two fire dozers; and the district operations center, staffed by multiple chief officers; resulted in rapid and overwhelming responses, which served to limit fire spread, and resultant damage when fires did occur.
All 60-plus grass and exterior fires were kept small, limiting potential for structure damage as a result of rapid and overwhelming responses as well as early notifications to 911 by residents.
Read More
The Jazz, Blues, and Funk Festival is BACK!
Join us at the Pittsburg Civic Center for the Jazz, Blues, Funk Festival the weekend of August 19-20. The Festival is a two-day event that will feature a variety of artists, food, beer, and wine.
Tickets are on sale now with the option for VIP, General admission, and Two-day Passes.
Buy your tickets now: www.pittsburgtickets.com
Read More
By Mashie Goldshmid, Program Director, Chabad of the Delta
With gratitude to G-d, we are excited to share that Chabad has just leased a new space to serve as the Jewish Center of East Contra Costa. The grand opening celebration will take place on Sunday, July 16 at 9:30am, inviting families and friends to join in the festivities.
The grand opening event promises an exciting lineup of activities for attendees of all ages. Live music performances, engaging kids’ entertainment, and a delectable dairy buffet are among the highlights that will contribute to the festive atmosphere. The celebration embodies the spirit of growth and community, inviting everyone to participate and rejoice together.
The new Chabad Jewish Center symbolizes a space where the East Contra Costa Jewish community can thrive collectively, creating an environment that encourages unity and embraces Jewish traditions. To RSVP visit JewishDelta.com/GrandOpening
Read More
Poor choices behind the wheel result in tragedy on California’s roadways
By Jaime Coffee, CHP Media Relations
SACRAMENTO, Calif. – The results of the California Highway Patrol’s (CHP) recent Independence Day Maximum Enforcement Period (MEP) are a sobering reminder of the consequences resulting from unsafe driving behaviors.
Sixty-eight people were killed in crashes throughout the state during the Independence Day MEP, which began at 6:01 p.m. on Friday, June 30, and concluded at 11:59 p.m. on Tuesday, July 4. Tragically, nearly half of the total number of vehicle occupants who died within CHP jurisdiction were not wearing a seat belt.
With unsafe speed being the number one contributor to crashes in California, the CHP placed a special emphasis on its enforcement during the recent MEP. CHP officers issued more than 9,700 speed citations throughout the long Independence Day weekend.
Additionally, impaired drivers were removed from California’s roadways at an alarming rate during the holiday enforcement effort. CHP officers made 1,224 arrests for driving under the influence, which is an average of one DUI arrest every five minutes.
“The results of this MEP are concerning and reinforce the need for responsible behavior behind the wheel,” said CHP Commissioner Sean Duryee. “All of these deaths were preventable, and the loved ones they leave behind will be forever impacted. Traffic safety is everyone’s responsibility, and these statistics show us how much work there is still to be done. The CHP is committed to making California’s roadways safer for all who use them.”
To help protect those who are traveling on California’s roadways during the holidays, the CHP implements six MEPs per year. The next MEP is scheduled for Labor Day weekend. Throughout the holiday weekend, all available uniformed members of the Department will be on patrol to enhance public safety, deter unsafe driving behavior, and, when necessary, take appropriate enforcement action.
Keep yourself and others who are on the road safe by buckling up, driving at a speed safe for conditions, avoid distractions behind the wheel, and always designating a sober driver.
The mission of the CHP is to provide the highest level of Safety, Service, and Security.
Read More
Enjoy parks safely and responsibly; no fireworks allowed in Regional Parks
The East Bay Regional Park District is urging Fourth of July visitors to enjoy parks safely and responsibly.
The Fourth of July holiday is typically one of the busiest days of the year for Regional Parks. Some of our more popular parks and swim areas are expected to reach capacity early in the day. Visitors are encouraged to carpool and arrive early. Parking lots may become full, though there are many Regional Park options to consider.
When visiting a Regional Park on the Fourth of July, visitors should know and follow these important tips and rules.
- NO Fireworks – Fireworks are not allowed in Regional Parks.
- Stay Cool and Hydrated – Plan ahead and bring plenty of water.
- Beat the Heat – With hot weather, visit in the morning and early evening when it is cooler. If you do venture out, wear a hat and loose, lightweight, and light-colored clothing.
- Drink Responsibly – Drinking alcohol is only allowed at certain Regional Parks. Check www.ebparks.org/parks before you go.
- Follow Water Safety Rules if Swimming – Free loaner life jackets are available at all East Bay Regional Park District swim facilities as an extra safeguard for anyone concerned about their swimming abilities or their children.
- Be Fire Smart – Be aware of Red Flag warnings, fire danger levels, and fire safety rules. www.ebparks.org/public-safety/fire/fire-danger-levels-restrictions.
The East Bay Regional Park District is the largest regional park system in the nation, comprising 73 parks, 55 miles of shoreline, and over 1,300 miles of trails for hiking, biking, horseback riding, and environmental education. The Park District receives more than 25 million visits annually throughout Alameda and Contra Costa counties in the San Francisco Bay Area.
Read More
By City of Pinole
The City of Pinole will not be hosting fireworks this year.
We encourage residents to enjoy a safe and fun Fourth of July, celebrating the birth of our exceptional nation. Families and friends often gather to recognize this special day together.
For a number of years, until 2010, the City hosted a fireworks display at Bayfront Park on Fourth of July. The City had been hoping to again host fireworks on Fourth of July in 2023. After collaborating with partner agencies to assess Bayfront Park and other sites, it was determined that there is no safe and accessible site in Pinole from which to launch fireworks. Since Pinole last held fireworks, fireworks safety standards and practices have evolved and concern about wildfires has increased substantially.
For those who would like to see fireworks, below is a list of events in Pinole’s neighboring cities.
3rd of July Fireworks
Richmond: Richmond Marina Bay Park, fireworks begin at 9:15 p.m.
Fourth of July Fireworks
Antioch: Fireworks in downtown Antioch over the San Joaquin River, start at after dusk
Concord: Mt. Diablo High School, at around 9 p.m.
Hercules: Bayfront Blvd, the show will start once it’s dark
Pleasant Hill: College Park High School fields, fireworks around 8:45 p.m.
Read More